Name | birth date | ||||
| date | |||||
| Oral aspects | |||||
| dryness | night | day | |||
| burning | |||||
| taste | normal | decreased | abnormal | ||
| periodontium | complaints | ||||
| prosthesis | adequate | failure | wearing overnight | ||
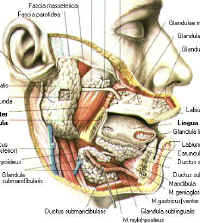
| Salivary glands | |||||
| Parotid | swelling L/R | pain | |||
| Submandibular | swelling L/R | ||||
Tr.respiratorius |
| ||||
COPD | |||||
Tr.digestivus | |||||
swallowing | impaired | ||||
maagklachten | diarrhee | obstipatie | |||
Tr.circulatorius | |||||
blood pressure | pulse | dizziness | nycturia | ||
vasc. accident | famil y | ||||
extremity ies | edem a | ||||
Tr.urogenit. | |||||
| cystitis | pruritis | menopau se | |||
disease of the joints | skin affections |
| |||
| Senses | taste disorders | ||||
| eye dryness | burning | ||||
| Metabolism | |||||
| diabetes | thyroid function | family | |||
| Allergic reactions | |||||
| Cranial trauma | |||||
| Surgery | irradiation | ||||
| Medication | chemotherapy | contraception | |||
| Intoxication | smoking N= | alcoholics E/dg | |||
| Remarks | |||||
Tools. Vacuum pump: (Atmolit). Adjust the pressure to minus 200 millibar. Coupling with a two way joint to enable bilateral saliva collection in one session. Use fine bore polythene tubing. (Portex, Hythe, Kent. England CT21 6JL Smith Industries.Ref. 800/100/420/100) Diameter: inside 1,57 mm. outside 2,08 mm. Length 30 m. There is some flow resistance due to adherence properties. A minimum salivary pressure of about 1 cm water is required. Collection cups according to Lashley, custom made. Outside 16 mm. Outer circle 1,5 mm. Height 4,5 - 6 mm. suitable for sterilization. Chronometer. Blood pressure meter. Stimulus: citric acid 5%. If indicated: pilocarpine HCl 5 mgr. capsule How to collect parotid saliva. Fixed time, preferable in the morning. The patient in upright position. Place the collecting cups carefully centrally in the papilla. By stretching the cheek and finger pressure outside the papilla will protrude in the oral cavity. Lead the collecting tubes always downward. Otherwise mechanical stimulation of the flow rate may occur. Record
Press the gland once only while collecting saliva. In cases of ductectasy a sudden wave (5 - 10 cm) is observed due to saliva pooling. Furthermore swallowing will activate the gland by a pharyngeal stimulus
The time lapse between stimulus and emerging of saliva in the collecting tube. Normal. ca. 20 sec. Not exceeding 60 sec. (citric acid) Increase. Small glands, loss of function, anticholinergic medication, ductectasy, "non-sal-saliva" (see sodium) Decrease. Intra cerebral stimulation, degeneration or intoxication. Cholinergic drugs, pilocarpine. Clinical. Relevant in the evaluation of dry mouth. A latency > 1 min. means discontinuity in salivary flow. The first portion may have a milky appearance. There is a good relationship between latency and flow rate:
The critical turn at 1 minute latency matches a flow rate < 0,3 ml/min. Normal values. Resting saliva. 0,05 - ,01 ml/min/gland. Increase. Local irritation (oropharyngeal), gingivitis/stomatitis, tumours, intra cerebral stimulation, c.q. dysregulation and degeneration (speech), n. vagus stimulation (stomach) and intoxications (Hg) Decrease. Small or aplastic gland. Tissue damage by inflammation, irradiation, Sjögren's disease. Ductectasy. Anticholinergics. In elderly people resting saliva me be diminished while normal stimulated volumes are produced. Stimulated function. 0,3 - 1,5 ml/min/gland. (citric acid) Increase. Large gland. Peripheral irritating factors. Intra glandular pressure caused by interstitial swelling from sialadenosis. Partial duct obstruction by hypertrophy of the m. masseter. Decrease. Tissue destruction by inflammation or irradiation. Anticholinergic drugs. Diminished perfusion due to dehydration and especially cardiovascular dysregulation. (with high as well as low blood pressure)
i.e. The number of the osmotic active particles in a solution (ions and molecules). If the concentration of the particles on both sides of a semipermeable differs a osmotic water transport will follow to compensate for it. This transport mechanism exerts an osmotic pressure on the membrane c.q. the semipermeable ductal lining. As the concentration within the duct is low, a water transport to the interstitium may follow. The osmotic pressure if present may cause ductectasy. Osmolarity = mOsmol/l (mmol/L.) Normal values. Osmolality = mOsmol/kg. (mmol/kg.) In blood 278-300 mmol/kg. In saliva 40 100 mmol/kg. In saliva among others ions, urea and proteins are active. Normally the osmolality varies between 40 in the (resting state) and 100 mmol/kg. (after stimulating). Acinar (primary saliva is supposed iso-osmotic to blood. Modulation. Striated duct: decreasing due to active transport of sodium and chloride to the surrounding tissue. Parotid duct: no changes i.e. impermeability for water and small solutes. In steady state about 40 mmol/kg. Pathology. Damage to the striated duct with failing reabsorption capacity. No decrease can be expected. Damage to the parotid duct initiates water transport outwards. The osmolality of the terminal saliva rises to serum values. (Mumps, Sjögren's, allergy). In time ductectasy will flow, thus continuing the state of inflammation. A sequence of water transport is increase of the concentration of large molecules: the proteins. Clinical. Raised in cases of damage, inflammation, allergy or hyper salivation (> 100 mmol/kg). Dropped in resting saliva and shortage of blood perfusion. Passive production. Paracellular together with water from the interstitial vessels via the intercellular "tight junctions". Transcellular via selective sodium channels:
Active production. Membrane transport with the help of membrane proteins and against the electro chemical gradients by means of the so called K-Na-ATP-ase pump. In this active exchange potassium enters the duct via potassium channels causing a K-gradient. This process needs intracellular chloride. It thereby overcomes the intra cellular sodium concentration of ca. 15 mmol/L. and potassium concentration of 150 mmol/l resulting in a primary saliva isotonic to serum. (sodium 136-146 mmol/L. and potassium 3,9-5 mmol/L.). Modulation. Within the striated duct the saliva is subject to active basolateral sodium transport generated through the K-Na-pump system. In the course of time the sodium concentration is decreasing. In the same process the potassium concentration increases. The exchange is time consuming and for sodium direct related to the flow rate. In resting saliva a steady state may be achieved where sodium values of 1-2 mmol/l and potassium up to 40 mmol/l. In the sound parotid duct some equilibration is possible dependent on the (im)permeability of the lining.
Normal values. There are no normal values. They are plotted against the given flow rate. There proportional relation is given in the function:
where x = the flow rate in ml/min. and f(x) = the sodium concentration in mmol/l. Disproportional high sodium values are to be expected if:
Clinical. Infection: mumps, cytomegalovirus, chronic obstructive inflammation. Irradiation. Gout? Allergy: butazolidine, furantoin.
Disproportional low sodium appears in:
The use of lithium may eventually mimic sodium behavior by competing the sodium transport channels. Clinical. Cardiovascular diseases with hypertension (atherosclerosis), dehydration, enlarged mean corpuscular volume (MCV) in cases with vitamin B 12 depletion, hypo tension and the use of drugs like lithium carbonate. The impact on the glands is systemic in nature and always bilateral . If not: the heterolateral gland has local problems like an inflammation which may show up as a result of longstanding dysfunction. This may be the dominant cause of chronic recurrent obstructive parotitis.
It is important to realize that a decreased flow rate using anticholinergic drugs shows a proportional behavior of sodium. Such a course may also be expected in small salivary glands. Source. Passive, acinar via second messager operated K-channels. In primary isotonic saliva a concentration of ca 4,5 mmol/l. can be measured. (blood 3,9 - 5 mmol/L. and intracellelular 150 mmol/L.) Active, by means of the K-Na-ATP-ase pump. Normal values. 20 - 30 mmol/L. There is a K transients phenomenon: the first portion of activated saliva shows higher values. Discarding the first portion or portions larger then 3 ml. is the right way to obtain reliable results. Modulation. The pump mechanism generates potassium in the striated duct up to 20 - 30 mmol/L. and in steady state even 50 mmol/L. Pathology. Sharp increase may be seen after digitalization. A decrease will follow damage to the striated duct in Sjögren's syndrome and (intra cellular) viral infection (mumps). Typical below 18 mmol/L. Source. Acinar cells, especially in the parotid gland. Modulation. During passage of the striated duct, along with sodium and chloride. Normal values. Inversely proportional to the flow rate. 1 - 35 mmol/L. (serum 22 - 28 mmol/L.) Clinical. Provides quantitative important buffer capacity, together with proteins and urea. It might be considered as an indicator for acinar energetic processes. Pathology. Bicarbonate is found consistent low level in "non-sal-saliva", not related to flow rates. In Sjögren's syndrome sometimes low values are seen shared with high sodium concentrations. (alfa-) amylase. 6 iso-enzymes exist. Determination according to enzymtechniques cf. the I.F.C.C. Source. 70 - 80 % of the amylase in total saliva is produced by the acinar cells of the parotid glands. Minor sources are the palatinal, sublingual and von Ebner's glands. The protein chain contains 512 amino acids. Molecule mass 56.500. Sugar chains are linked to it in about 25 %. The production is initiated by a beta adrenergic stimulus. Normal values.
Concentration. Varies between 70.000 and 800.000. The concentration increases due to water reabsorption in the striated duct and osmotic transport out of the parotid duct. Elevated values come out in resting saliva or after beta mimetic stimulation (drugs). Longstanding dietary habits (starch) may produce substantial increase. Production pro minute. Normally > 100 U/min. The production pro minute eliminates the epithelial water transport thus giving a correct idea of the acinar activity. Decrease. After irradiation and in Sjögren's syndrome. Intoxications like by digitalis or beta blockers and in anorexia or a lack of amino-acids. Increase. All stimuli with (beta-)adrenergic activity. Chewing itself and medication with pilocarpine. Clinical. In Sjögren's syndrome initially a decreased production pro minute goes together with an increased concentration as a consequence the loss of water through the permeable duct lining. Source. Acinar cells. The individual gland types produce different quantities and qualities. Parotid saliva contains alpha-amylase, acid and basic PRP's (proline rich protein), s-IgA (secretory IgA), proline rich glycoprotein, cystatin, statherin, histatin, gustin and lysozym. In the submandibular saliva: mucines, PRP's, amylase, growth factors. The molecular mass varies and may be large. Production. The production needs a (beta-)adrenergic stimulus. Pilocarpine has also adrenergic side effects. Food habits are relevant and may enhance the protein output substantially. Modulation. Proteins hardly pass the duct lining. Therefore the concentration is highly dependant on the transepithelial water transport. Increasing values are seen due not only to increased water reabsorption in the striate duct (resting saliva) but also to waterloss from the parotid duct during inflammation. Apart from the concentration the production pro minute ( mg/min. = g/L. x ml/min.) is a usefully parameter for the vital capacity of the gland. Pathology. The production decreases after destruction of the acinar cells. In malignancy abnormal proteins are seen. Albumin appears due to increasing duct permeability. Clinical. Low values of production pro minute are seen after irradiation and Sjögren's disease, in the initial phase along with increased concentrations. Drugs with adrenergic activity increase the production, while an abnormal or disturbed protein synthesis causes swelling of the acinar cells. This is a characteristic feature in sialadenosis. In resting saliva strikingly high protein concentrations appear due to active water reabsorption. Urea in saliva Source. The liver (see also urea in blood) It is a small neutral molecule. Mass: 60 (water 18) with the formula CO(NH2)2. In the acini it is subject to ultra filtration. In normal tissue a some molecule reflection may be expected. Therefore the ratio salivary urea/ serum urea < 1. Modulation. Always passive and dependant on transepithelial water transport. Concentration increase in the striated duct leads to an inverse saliva/blood ratio: salivary urea/serum urea > 1 if: flow rate < 0.3 ml/min. Pathology. Small damage to the parotid duct may cause an increase of the urea concentration, following osmotic water transport, while in serious permeability urea is also filtered. In Sjögren's disease the result of the reverse activities in unpredictable and dependant of:
a. loss of striated duct water reabsorption. b. degree of permeability of the parotid duct. Clinical. A saliva/serum ratio > 1 is found in resting saliva (< 0.3 ml/min.) as well as in "non-sal-saliva" Oral activity. Degrading of urea by bacterial urease leads to an alkalinization of the environment. CO(NH2)2 H2O => CO2 2NH3 This means buffer capacity to acids adding up with bicarbonate. Active microorganisms are:
Hematology.
(alfa-)Amylase (U/L)
Source. Iso-enzymes are produced by the pancreas as well as by the salivary glands.
Normal values differ by the investigation technique. Catharinahospital Eindhoven NL (CZ): < 175 U/L.
Pathology. Increasing values in pancreatitis, cholecystitis, opiates, mumps, acute allergic reactions of the parotid gland. Salivary stones with obstructive adenitis. Adenocarcinoma in the lung may produce salivary amylases.
Clinical. Irradiation is followed by a sharp rise of the serum amylase. Prolonged dosage reduce the concentration. A good indication of the salivary amylase activity is given by:
salivary amylase = total amylase minus pancreatic amylase The pancreatic amylase is encoded by a gen on the first chromosome. It differs from salivary amylase. Source. The pancreatic gland. 94% is homologous to salivary amylase. It lacks sugar chains. Adult levels are reached after the age of 10 - 15. The normal stimulus is cholinergic. Normal values (CZ): < 90 U/L. Increase suspect for pancreatic tumor. Salivary amylase in serum (U/L) Some leakage of salivary amylase to the bloodstream is seen even under normal conditions. It amounts about 1/10.000 of the parotid concentration. No routine direct measurement is available. However a good estimation of the total salivary amylase activity is possible an found by: salivary amylase = serum amylase minus pancreatic amylase Normal values. 20 - 70 U/L. Pathology. An increase is seen after a sudden obstruction of the gland due to salivary calculus and in the initial phase of irradiation. Decrease (to zero) indicates a loss of acinar function as seen in Sjögren's syndrome and after prolonged irradiation. In fact is the measurement of salivary amylase in serum the easy way evaluate the stage of a destructive process. Clinical. After total acinar loss negative figures are sometimes found due to laboratory variables. Source. The liver. After digestion food proteins are degraded to amino acids in the liver. The side product ammonia is immediately synthesized to urea: 2NH3CO2 ---> CO(NH2)2. In renal elimination 40 - 50 % is reabsorbed. Normal values. in serum: 3,3 - 6,7 mmol/L. Modulation. Increase related to food and protein uptake, rapid tissue destruction, or impaired kidney function. Low concentrations appear during growth, adolescence, gravidity and low protein uptake. Clinical. Information about serum urea is essential in evaluation of the water transfer. Source. Uric acid is a main final product of the purine metabolism. Normal excretion via filtration in the kidney (where 90% reabsorption). The solubility at pH < 7,4 is low. Metabolic increase follows elevated uptake of nucleinic acids in the blood circulation after consumption (meat, sherry) High values are found in gout. Interaction occurs with drugs like allopurinol, cortison, dicoumarol. Indication for diagnostic test. Gout, impaired renal function. Normal values. 0.12 - 0.36 mmol/L. Clinical. High levels > 50 mmol/L tend to crystallization. If crystals are present in the parotid gland it mimics inflammation. Registration of the arterial tension should be a standard procedure. Its meaning lies in the impact of hypertension on the microcirculation. The normal parotid effort after stimulation requires a 20 fold increase of blood perfusion. If absent a "non-sal-saliva" response can be expected. In reverse this phenomenon is suspect for hypertension and hypercholesterolemia. Hypertension should verified on both left and right side. A single finding of high blood pressure is related to 50% chance on hypertension. Salivary pressure. (cm. water column) There no obvious relation between the salivary pressure and blood pressure. The first is mainly generated by myo-epithelial contraction. Perhaps is the protein osmotic force contributive. Normal value. 10 -40 cm water column. Technique. Hold the collection tube upright. Wait for a steady state. Increase. Large glands. Also in "non-sal-saliva" due to simultaneously activation of a larger number of secretory units. All forms of slight counterpressure cause an unilateral increase of the flow rate. Decrease. Damage , inflammation, ductectasy. Clinical. A persistent counter pressure of the gland is to be expected in hypertrophy of the masseteric muscles. Interstitial swelling as in sialadenosis may also cause some counter pressure and explains the incidental finding of elevated flow rates Additional investigations. Sedimentation rate (ESR) Exploration of inflammation or an active immunologic process. Leucocytes. Infection, inflammation, allergic states. Mean Corpuscular Volume (MCV) 88 - 100 fL. Increase of the cell volume impairs the capillary blood flow and leads to "non-sal-saliva" Values > 100 fL. require further determination of vitamin B 12 and folic acid. Hepatic parameters. Alkaline phosfatase (30-11 U/L.), gamma-glutamyl-transpeptidase (g-GT) (< 35 U/L. man, < 24 U/L. woman) and alanin-amino-transferase (ALAT) (< 35 U/L.) Elevated g-GT is suggestive for alcohol abuse, simultaneous rise of ALAT indicates permanent damage. Verify deficiency of vitamin B12. Total protein. (61-80 g/L. adult) and its differentiation. Relevant to inflammation and auto-immune activity. High values of gamma globulins in Sjögren's syndrome. Antinuclear antibodies (ANA). If positive follows differentiation to ENA (Extractable NA) including SS-A (anti Ro) and SS-B (anti La) antibodies. Positive SS-A (frequently) and SS-B (sometimes) is suspected for Sjögren's syndrome. Disappearing may announce a non-Hodgkin lymphoma. Cholesterol. (3,5 - 6,5 mmol/L.adult) Predictive factor in pathology of the blood vessels. complete the investigation with LDL and HDL. Essential in relation to "non-sal-saliva". Thyroid stimulating hormone (TSH) (0,2 - 5,5 mU/L.) The values are reverse to thyroid activity. Usefully to exclude auto-immune thyroiditis in Sjögren's syndrome and especially in bilateral symptom free swelling of the submandibular gland. Incidentally after irradiation and in evaluating taste disorders ( and thyroid depressing drugs). june 2000
|
|